What do you know about epidurals and their risk and benefits? In this blog (Part 1) , Dr Buckley explores the impacts of epidural on oxytocin and the flow of labour, and what this might mean for … [Read more...] about Epidurals in Labour (Part 1)
Blog
2017: Reasons for Hope

From the personal and local, to the national and global, things seem to be getting more extreme and polarised, and it can be easy to sink into despair and hopelessness. Please remember that we have … [Read more...] about 2017: Reasons for Hope
Gentle, Natural, Mammalian Birth

In the festive season, we celebrate perhaps the most famous gentle, natural, birth in history. Blessed Mary gave birth to her legendary baby in the most low-technology setting imaginable... and … [Read more...] about Gentle, Natural, Mammalian Birth
Normal Labour and Birth Conference, Sydney 2016: Science, Love and Dancing!
The International Normal Labour and Birth Conference, downunder for the first time this October (2016), was, as one participant described, "A perfect blend of science, love, and dancing.” It was a … [Read more...] about Normal Labour and Birth Conference, Sydney 2016: Science, Love and Dancing!
Ultrasound Scans in Pregnancy – Your Questions Answered!

Having an ultrasound has become an expected part of pregnancy, and modern women may have many scans, sometimes beginning from the early weeks. We are also lining up for “keepsake” scans, where we are … [Read more...] about Ultrasound Scans in Pregnancy – Your Questions Answered!
What to Eat When You’re Expecting to be Expecting

This is it! You’re pulling out all the stops, ditching the rubber, trashing the pills, popping out the birth-control implants, un-inserting the IUDs and everything else that stands between … [Read more...] about What to Eat When You’re Expecting to be Expecting
Five Tips for Fertile Fun
You’re wanting to make a baby. Congratulations on taking the first steps on your journey to family! You are probably wondering exactly what you are supposed to be doing. Or not doing? Is it … [Read more...] about Five Tips for Fertile Fun
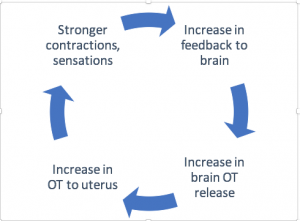
What’s so Great about Hormonal Physiology?

Hormonal physiology describes the healthy functioning of our hormonal systems. My new report Hormonal Physiology of Childbearing provides scientific evidence and detail about these processes in … [Read more...] about What’s so Great about Hormonal Physiology?
Hormonal Physiology of Childbirth: How to eat an elephant

"This report, prepared by Dr. Sarah Buckley in collaboration with Childbirth Connection Programs at the National Partnership for Women & Families, will be retrospectively evaluated as one of the … [Read more...] about Hormonal Physiology of Childbirth: How to eat an elephant
Hormonal Physiology of Childbearing Report

• How are labour and birth designed to work for mother and baby?• What processes ensure that both make the safest and easiest transitions from pregnancy to postpartum?• Are there important … [Read more...] about Hormonal Physiology of Childbearing Report

 Discover the science and pleasure of Ecstatic Birth!
Discover the science and pleasure of Ecstatic Birth!